⭐⭐⭐ KIDNEY STONES ⭐⭐⭐
⭐⭐⭐ KIDNEY STONES ⭐⭐⭐
1) DEFINITION OF KIDNEY STONES:-
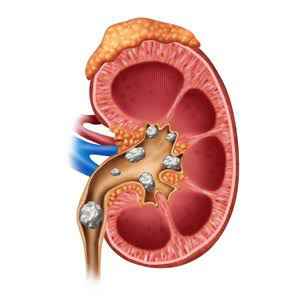
Kidney stones are hard, pebble-like pieces of material that form in one or both of your kidneys .





 Triple phosphate stone crystal - Coffin lid shaped.
Triple phosphate stone crystal - Coffin lid shaped.








1) DEFINITION OF KIDNEY STONES:-
Kidney stones are hard, pebble-like pieces of material that form in one or both of your kidneys .
2) CAUSES OF KIDNEY STONES :-
(I) Hyperparathyroidism :- i.e increased production of parathyroid hormone.
- Hyperparathyroidism leads to hypercalcaemia i.e increased levels of calcium in the blood. This extra Calcium enters the kidney for excretion. Thus, increased concentration of calcium in kidney leads to formation of kidney stones.
- Hyperparathyroidism causes hypercalcaemia because PTH hormone causes increased renal resorption of calcium, increased synthesis of active form of vitamin D (which increases intestinal calcium absorption), and increased resorption of the bone.
- Following conditions can cause hyperparathyroidism :-
# Noncancerous growth or cancerous growth or hyperplasia of parathyroid gland.
# Severe calcium deficiency - low blood calcium stimulates parathyroid gland.
# Vitamin D deficiency ( vit D causes absorption of calcium from intestine) - vit D deficiency causes decreased levels of calcium in blood.
# Chronic kidney failure
( kidney converts 25 hydroxy Vit D3 into
1, 25 dihydroxy vit D3 i.e active form of vitamin D)
⭐⭐⭐⭐
(II) Increased glycine metabolism :-
One metabolic pathway for glycine leads to glyoxylate which is the precursor of oxalate.
Oxalate synthesis is a critical factor in calcium oxalate urolithiasis.
⭐⭐⭐⭐
(III) Cystinuria
- Cystinuria is inherited in an autosomal recessive pattern. Mutations in some genes result in the abnormal transport of cystine in the kidney . Excess cystine in the urine can lead to the formation of crystals and stones.
⭐⭐⭐⭐
(IV) Low urinary citrate excretion or hypocitraturia :-
- Citrate inhibits stone formation by complexing with calcium in the urine, inhibiting spontaneous nucleation, and preventing growth of crystals of calcium oxalate and calcium phosphate.
Hypocitraturia, i.e low amount of citrate in the urine, is an important risk factor for kidney stone formation.
- Hypocitraturia ( less citrate in urine ) may be caused by
# Idiopathic
# Metabolic acidosis, renal tubular acidosis -
Citrate can be metabolized to bicarbonate and thus it acts as a base .
During acidosis, citrate gets used up due to its action as base and hence it's excretion in urine decreases.
# Hypokalemia -
- Hypokalemia produces intracellular acidosis because potassium move from cells to extracellular fluid (plasma) in exchange for hydrogen ions.
- ( Potassium is more in cells compared to ECF. Hypokalemia i.e decreased amount of potassium in plasma further increases the concentration gradient of potassium between cell and plasma. Hence K ions move out of cells and H ions enter the cell leading to intracellular acidosis )
Hypokalemia causes decrease in tubular pH. This results in increased citrate uptake and metabolism to neutralize the acid.
# Androgens
# Dehydration - it can cause acidosis due to loss of fluid and increased concentration of H ions. This acidosis causes consumption of citrate.
# Thiazide diuretics - thiazides can lower urine citrate, because they deplete potassium stores in cells and lower the pH inside kidney cells ( see above point of hypokalemia to understand how hypokalemia causes intracellular acidosis and how acidosis causes consumption of citrate)
# carbonic anhydrase inhibitors like acetazolamide - It causes acidosis by reducing bicarbonate reabsorption in the proximal renal tubule. (Bicarbonate is base.)
# Diarrhea also causes direct gastrointestinal loss of citrate and magnesium.
# high protein intake,
- Diets high in animal protein provide an acid load. This promotes mild metabolic acidosis,
# exercise, - acidosis during intense exercise can be caused by the increased production of lactic acid,
# starvation -Starvation usually produces a mild metabolic acidosis, due to production of excessive ketone bodies (acetone, acetoacetic acid, and beta hydroxybutyric acid) during the process of fat decomposition as glucose is not available.
# urinary tract infection (probably because of bacterial degradation of citrate).
⭐⭐⭐⭐
(V) Urinary tract Infection by urea splitting bacteria :-
Bacterial urease splits urea and promotes the formation of ammonia and carbon dioxide leading to urine alkalinization and formation of phosphate salts of ammonium , magnesium. - struvite stones
⭐⭐⭐⭐
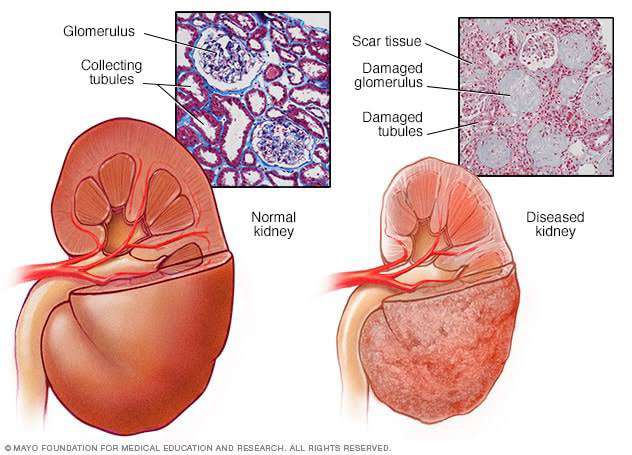
(VI) Medullary sponge kidney :-
It is a congenital disorder of the kidneys characterized by cystic dilatation of the collecting tubules in one or both kidneys.
The cysts cause the collecting tubules to become wider . This makes the drainage of urine slow and inefficient leading to stasis of urine. Waste products such as excess calcium build up in the kidneys. This can result in formation of kidney stones.
⭐⭐⭐⭐
(VII) Any obstruction which leads to stasis of urine :-
Various anatomical obstructions promote urine stasis and increase the risk of stone formation by promoting precipitation of crystals.
⭐⭐⭐⭐
(VIII) Vitamin A deficiency :-
Vitamin A deficiency leads to
(a) Reduced concentration of crystal growth inhibitors, i.e citrate and glycosaminoglycans;
(b) Increased concentration of stone forming factors, like calcium and oxalate.
⭐⭐⭐⭐
(IX) Chronic immobilisation :-
- Prolonged immobilization interferes with the drainage of urine from the pelvis and calyces due to the position occupied by kidneys.
- This provides sufficient time for the deposition and retention of crystals thus leading to calculus formation.
- In addition to this, stasis may also promote infection by urea splitting bacteria which may further promote calculus formation.
⭐⭐⭐⭐
(X) In summer, dehydration occurs due to increased temperature. Dehydration leads to constant low urine volume. When urine volume is low, urine is concentrated . Thus Increased concentration of stone forming substances favours crystal deposition.
⭐⭐⭐⭐
(XI) Conditions like hypercalciuria, hypervitaminosis D, gout , hypomagnesemia can lead to kidney stone formation.
- Hypercalciuria leads to increased concentration of calcium in urine thus favouring crystal formation.
- Hypervitaminosis D means increased concentration of vitamin D.
Vitamin D increases absorption of calcium from intestine. This leads to hypercalcaemia and hypercalciuria.
- gout is characterized by increased concentration of uric acid . Hence, there is higher risk of developing uric acid stones because higher level of uric acid is being excreted by the kidneys.
- hypomagnesemia
Magnesium inhibits calcium oxalate crystallization in urine. Magnesium inhibits absorption of dietary oxalate from the gut lumen. Hence , hypomagnesemia favours crystal formation.
⭐⭐⭐⭐
(XII) Randall's theory :-
- It states that crystals of minerals are passed out through urine. If these crystals are large, they are not passed out through urine. They get adhered to the urothelium causing subepithelial plaque.
This plaque acts as a nidus for stone formation.
⭐⭐⭐⭐
3) STEPS IN STONE FORMATION :-
(I) Supersaturation.
(II) Nucleus formation.
(III) Crystal formation.
(IV) Aggregation.
(V) Matrix formation.
(VI) Stone formation.
4) TYPES OF KIDNEY STONES :-
(I) Oxalate stones :- 75℅
# Calcium oxalate stones.
#Mulberry stones - Brown coloured and with multiple projections.
# Calcium oxalate monohydrate crystal-
Dumbell shaped.
(II) Calcium oxalate dihydrate crystals - envelope shaped.
(II) Phosphate stones :- 10-15℅
# Made of Calcium Phosphate or Magnesium, Ammonium Phosphate, in the infected urine.
# It is smooth, white & radiopaque.
# Sometimes, it enlarges rapidly & take shape of renal calyces - Staghorn stone or
Struvite stones .
# It is formed due to urea splitting organisms like Klebsiella, Proteus. (See the point in etiology of kidney stones)
# Consist of Carbonate, Ammonium, Magnesium, Phosphate (CAMP).
(III) Uric acid stones :- 5%
# Formed in gout, uricosuria.
# Yellowish, translucent, hard & smooth. They may be of any shape.
(IV) Cystine stones :-
# Seen in Cystinuria (autosomal recessive). See etiology for explanation.
# Seen in young girls with acidic urine.
# Stones are yellow, smooth, multiple, radiopaque (due to sulphur present in cystine) which become greenish on exposure.
Cystine stones - Hexagonal.
(V) Indigo stones :-
# Very rare.
# Blue in colour.
(VI) Xanthine stones :-
# Formed due to deficiency of Xanthine Oxidase. Insoluble xanthine in urine forms stones.
# Brick red coloured, smooth.
5) CLINICAL FEATURES OF KIDNEY STONES :-
(I) Pain
- Pain occurs in the regions of renal angle, hypochondriac and lumbar regions.
- It radiates to groin, testis, tip of penis in males.
- Pain may fluctuate on movement due to change in location of stone on movement of body.
- There may be vomiting. It occurs because of shared nerve connections between the kidneys and GI tract. Stones in the kidneys can trigger nerves in the GI tract.
- Capsule surrounding the kidney contains nerve fibers that transmit pain. Obstruction to the urine flow due to stone leads to stasis of urine. This backed up urine then causes swelling and expansion of the capsule which activates those nerve fibers, causing signals that are interpreted by the brain as an intense, visceral pain.
- When a stone is moving into the ureter, ureters contract as they try to push the stone out. This muscle spasm causes pain. Pain may be felt in flank, side, or back.
(reason why pain arises in muscle spasm is muscle ischemia, which leads to a drop in pH and the release of pain-producing substances such as bradykinin, ATP, and H+.)
Pain can also radiate to the groin and the front of thigh.
If the stone becomes lodged in the ureters, it may block the flow of urine and cause the kidney to swell and the ureter to spasm, which can be very painful.
- Once the stone has moved down to the part of the ureter closer to the bladder, pain is felt in the abdomen or groin.
- Pain can come and go as the body tries to get rid of the stone.
(II) Hematuria :- blood in urine
- As the stones grow they may eventually become large enough to irritate either the lining of the kidney or the ureter and cause injury to the local cells and capillaries causing hematuria.
(III) Pyuria :- pus in urine
- Stone coming down the urinary tract can cause inflammation and irritation of the ureter leading to Pyuria. Stasis of urine due to obstruction may also favour infection.
(IV) Fever :-
It indicates that infection has occurred due to urine stasis.
(V) There may be Oliguria , painful micturition, frequent urination due to kidney stone because of obstruction to the flow of urine.
(VI) Urinary tract Infection ( UTI) :-
- It can occur due to urinary stasis.
- May present with
Painful or burning micturition
Frequent urination
Pyuria
Oliguria
Fever
(VII) Hypertension :-
- Commonest of all stones is Calcium oxalate stones.
Alterations in calcium metabolism may play an important role in the pathogenesis of both kidney stones and hypertension .
( Calcium increases BP by causing contraction of vascular smooth muscle i.e vasoconstriction )
- Other cause of Hypertension may be following :- Tubular injury associated with kidney stones stimulates production of angiotensin in kidney.
(VIII) Tenderness in renal angle
(IX) There may be palpable mass in the loin due to hydronephrosis which is smooth, moves with respiration and ballotable.
⭐ Symptoms related to causes ⭐:-
(I) Hyperparathyroidism :- May present with :-
- Joint pain.
- Muscle weakness.
- Depression.
- Loss of appetite.
If hyperparathyroidism is more severe, there may be following symptoms:-
- Nausea and vomiting.
- Confusion
- Increased thirst and need to urinate.
- Constipation.
- Bone pain.
(II) Urinary tract Infection
May present with
Painful or burning micturition
Frequent urination
Pyuria
Oliguria
Fever
(III) Any obstruction in urinary tract which leads to stasis of urine :-
- Pain
- Obstruction that leads to hydronephrosis may cause digestive tract symptoms, such as nausea, vomiting, and abdominal pain.
- People who have urinary tract infections (UTIs) may have pus or blood in the urine, fever, and discomfort in the area of the bladder or kidneys.
- Obstruction can stop or reduce urination if blockage affects the ureters from both kidneys or if it affects the urethra.
- Obstruction of the urethra or bladder outlet may cause pain, pressure, and distention of the bladder.
(IV) Dehydration :-
Signs of dehydration may be present :-
- dark yellow urine
- feeling tired or dizzy
- dry mouth, lips and eyes.
- Oliguria
- Skin pinch test - skin fold requires long time to revert back to position after pinching.
(V) Hypercalcaemia
- Abdominal pain, kidney stones, excessive thirst, bone pain, muscle weakness and confusion, nausea.
Hypomagnesemia
May present with:-
- anorexia, nausea, vomiting,
- lethargy, weakness,
- personality change, tetany (eg, positive Trousseau or Chvostek sign or spontaneous carpopedal spasm, hyperreflexia),
- tremor and muscle fasciculations.
- It may also present with
Seizures, delirium or cardiovascular manifestations with ECG changes.
Gout
- Intense joint pain.
- Inflammation and redness of joint. The affected joints become swollen, tender, warm and red.
- Limited range of motion.
⭐⭐⭐⭐⭐⭐
6) INVESTIGATIONS OF KIDNEY STONES:-
(A) Investigations for diagnosis of kidney stones:-
(I) X ray KUB ( Kidney ureter bladder )- Radiopaque stones.
(II) USG Abdomen.
(III) CT scan.
(IV) IVU ( Intravenous urography )
- For kidney function & hydronephrosis.
(V) Retrograde pyelography.
(VI) Urine - Culture & Sensitivity to detect infection.
(VII) Blood test - Blood Urea, uric acid, Serum creatinine, Calcium, Phosphate, etc.
(VIII) Urine test -Detect Uric acid, Cystine, Calcium, pH, etc.
(B) Investigations related to causes of kidney stones :-
(I) Hyperparathyroidism :-
- Blood tests measuring the levels of parathyroid hormone (PTH), calcium .
- Urine Tests: Checking the urine during a 24-hour period can determine how much calcium the body is excreting.
- Bone Density Test: Looking at the bones detects any bone loss or weakening.
- X-ray, Ultrasound and CT scan: to identify any bone fractures.
(II) Increased glycine metabolism :-
( oxalate synthesis is increased)
- Urine tests to measure levels of oxalate ; urine is also checked for crystals.
- Blood test to measure the amount of oxalate in blood.
(III) Cystinuria :-
Screening for cystinuria should be considered in people with recurrent or bilateral (i.e. affecting both kidneys) stones; those who develop stones at an early age (before age 30); and people who have a family history of cystinuria. Urinanalysis and genetic testing can help in this case.
(IV) Hypocitraturia :-
Hypocitraturia - less than 320 mg of citrate excreted per 24-hour urine collection.
(V) Urinary tract Infection by urea splitting bacteria :-
May present with
Painful or burning micturition
Frequent urination
Pyuria
Oliguria
Fever
(VI) Medullary sponge kidney :-
USG and CT scan.
(VII) Any obstruction which leads to stasis of urine :- IVU
(VIII) Vitamin A deficiency :- other signs of vitamin A deficiency may be present.
(IX) Conditions like hypercalciuria, hypervitaminosis D, gout, hypomagnesemia
- Blood levels of calcium, Vit D , uric acid , Magnesium.
⭐⭐⭐⭐⭐⭐
7) TREATMENT OF KIDNEY STONES:-
(I) PCNL - Percutaneous Nephrolithotomy -
# Procedure - A needle is passed percutaneous through the loin into the kidney through USG or C arm guidance.
It is passed into the calyces & renal pelvis.
Then, a guidewire is passed.
Later, dilators are passed to widen the track.
Finally, a nephroscope is passed & with the help of ultrasonic energy the stone is fragmented & removed by suction.
# Indication -
Stones are > 2.5 cm.
If Multiple stones, ESWL is not useful.
# Complications -
- Damage to colon while producing track for nephroscope.
- Rupture of collecting duct.
- Hemorrhage.
(II) ESWL - Extracorporeal Shock Wave Lithotripsy -
# Procedure -
Stones are fragmented with help of electromagnetic shock waves. Medium of passage of shock is water bath/ cushion.
Shock waves = 2/sec.
1000-4000 waves for each stone.
Stones are located by USG or fluoroscopy.
# Advantages -
- No anaesthesia.
- It can be done repeatedly.
- Stones < 2.5 cm are easily fragmented.
- Hard oxalate stones are fragmented.
# Complications -
- Renal hematoma.
- Hematuria.
- Fragmented stone can lodge in ureter.
- Damage to adjacent tissues.
# Contraindications -
- Pregnancy.
- Patients with abdominal aneurysm.
- Bleeding disorders.
- Sepsis & renal failure.
(III) Conservative treatment -
# I.V. Fluids.
Increasing fluid flow through the affected kidney may help in stone passage, thereby improving symptoms more quickly.
It also decreases dehydration and it makes concentrated urine dilute. It also decreases acidity of urine.
# Inj. Furosemide.
Lasix blocks the absorption of sodium, chloride, and water from the kidney tubules, causing increase in the urine output which may help in passage of stone.
# Calcium channel blockers.- They stop the ureter from spasming, which helps relieve pain. They also help widen the ureter so the stone can pass more easily.
Alpha blockers - Alpha blockers relax the muscles in the ureter. This can help the stone pass more easily. Relaxing the muscles can also help relieve pain caused by spasms in the ureter.
# Anti inflammatory & antispasmodic agents to relieve pain due to spasm of ureter and inflammation ( which occurs due to stasis of urine)
# Flush therapy.
Increasing the amount of urine helps to flush the kidneys. Hence flush therapy helps in passage of stones. Drinking enough fluid will help keep your urine less concentrated with waste products.
# If you get calcium stones, a thiazide diuretic may be beneficial.
Hydrochlorothiazide decreases the amount of calcium in urine by increasing calcium reabsorption into the blood in exchange for sodium.Thus, thiazides reduce urine calcium levels and increase blood calcium.
# If you get uric acid stones, allopurinol can help reduce uric acid in your blood or urine.
# If you get struvite stones, long-term antibiotics may be used to help reduce the amount of bacteria present in your urine
# If you get cystine stones, Captopril may help reduce the level of cystine in your urine by formation of the captopril–cysteine disulfide which is more soluble in urine.
(IV) Surgery -
# Pyelolithotomy - (pyelo means renal pelvis, lithotomy means surgical removal of a calculus )
(When the stone is extra renal pelvis i.e pelvis outside the kidney )
Steps :-
- Incision is made through loin.
- Incisions in plevis.
- Stone is removed.
- Pelvis is closed.
# Extended pyelithotomy -
(When the stone is intra renal pelvis i.e pelvis inside the kidney )
Steps :-
- Incision is given at hilum (midway between pelvis & kidney) & stones are removed from pelvis & calyces.
# Nephrolithotomy - ( Nephro means kidney )
Incision made through loin into the kidney.
(at Brodel's line)
# Nephropyelolithotomy -
Incision is made in both pelvis & kidney.
# Bench surgery -
Kidney is removed temporarily & kept in ice packs or liquid nitrogen.
Stones are removed & kidney is replaced back in the body.
# Coagulum pyelolithotomy -
Coagulum solution containing fibrinogen is poured into renal pelvis. When it solidifies, it forms a mass entangled with stone. This whole mass is removed with stones.
# Partial nephrectomy -
Done if there are mutiple stones at one pole or damaged calyx.
8) PREVENTION OF KIDNEY STONES:- (I) Drinking enough water will keep your urine less concentrated with waste products.
(II) Sugar should be limited to small quantities.
(III) Eat more fruits and vegetables, which make the urine less acidic. Animal protein produces urine that has more acid, which can increase the risk for kidney stones.High urine acid may cause both uric acid and calcium oxalate kidney stones. Decrease consumption of animal protein.
(IV) Reduce salt intake :- Too much salt in the urine prevents calcium reabsorption from the urine to the blood. This causes high urine calcium, which may lead to kidney stones.
Eating less salt helps keep urine calcium levels lower.
(V) Eat dairy products having calcium. They actually help to prevent stones, because calcium binds with oxalate before it gets into the kidneys.
People with the lowest dietary calcium intake have an increased risk of kidney stones because there is no enough calcium to bind to the oxalate present in the blood. Hence oxalate accumulates in urine and increases risk of stone.
Low-calcium diets may increase your kidney stone risk .
But too much consumption should also not be done.
Calcium supplements, however, may increase your risk of stones. Hence, dietary calcium should be preferred rather than supplements.
(VI) Avoiding oxalate-rich foods may help prevent the stones from forming.
Foods high in oxalates are:
-

(VII) Taking certain medications can increase risk of kidney stones.
Some of these medications are:-
- Anticonvulsants like topiramate
steroids
- Chemotherapy drugs
- Uricosuric drugs
- Diuretics
- Antacids that contain calcium
- Supplements containing calcium
- Indinavir , a drug used in treating HIV infection
- Nasal decongestants
- Protease inhibitors
⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐

Waiting long time. Eager to read post. Nice in advance👌
ReplyDeleteThank you so much 😊😊
DeleteInclusion of pictures is the best thing👌👌Awesome as always.. Improving day by day. Keep it up
ReplyDeleteThank you so much 😊😊
DeleteGood topic very nice writing keep it up 👍👍👍👍
ReplyDeleteबरेच दिवस झाले आपल्या article ची वाट पाहत होतो अखेर एका चांगल्या टॉपिक Kidney Stones वरती एक छान लेख वाचायला मिळाला अगदी pictorial diagram सुद्धा पाहायला मिळाल्या. आपल्या लिखाणाला दाद द्यावी असे वाटते. आम्हा सर्वांना एका ब्लॉग वरती एवढ्या विस्तृत टॉपिक वरती थोडक्यात बरीचशी माहिती मिळते. तू अशीच लिहीत रहा जेणेकरून सर्व डॉक्टर्स याना याचा चांगला फायदा होईल. तुझ्या कष्टाला द्यावी लागेल तुला तुझ्या जीवनात याचा खूप फायदा होईल. माझ्या कडून तुला खूप शुभेच्छा.
ReplyDeleteThank you so much 😊😊
DeleteWonderful
ReplyDeleteThank you so much 😊😊
DeleteNice one
ReplyDeleteKhup chan lihile aahe. Article with pictures explains a lot. Nice article. Keep it up Dr. Nikita.👍👍👍
ReplyDeleteThank you so much 😊😊
Delete👌👌👌
ReplyDeleteThank you so much
Delete😊😊
DeleteGood
ReplyDeleteThank you so much 😊😊
DeleteNice
ReplyDeleteThank you so much 😊😊
DeleteGood post
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteNice one dr nikita
ReplyDeleteThank you so much 😊😊
DeleteKeep it up dear
ReplyDeleteThank you so much 😊😊
DeleteBeta 👌👌
ReplyDeleteThank you so much 😊😊
DeleteBadhiya
ReplyDelete😊😊
DeleteNicely done
ReplyDeleteThank you so much 😊😊
Deleteबेटा खुप मस्त
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteGreat
ReplyDeleteThank you so much 😊😊
Delete👌👌👌👌✨✨✨
ReplyDeleteThank you so much 😊😊
Delete👍👍
ReplyDeleteThank you so much 😊😊
Delete👍👍👍👍
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteGreat effort beta
ReplyDeleteThank you so much 😊😊
DeleteGud
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDelete