⭐⭐ AORTIC REGURGITATION ⭐⭐
1) AORTIC VALVE -
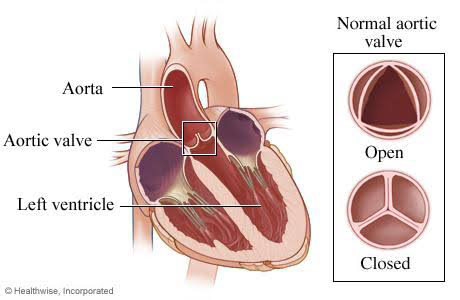
- Aortic valve is a semilunar valve present
between left ventricle and aorta. It
directs the flow of blood from left
ventricle into the aorta during
ventricular systole.
- During ventricular systole, pressure
rises in the left ventricle. When the
pressure in the left ventricle exceeds the
pressure in the aorta, the aortic valve
opens and the blood flows from the
left ventricle into the aorta.
⭐⭐⭐⭐⭐⭐⭐
2) DEFINITION OF AORTIC REGURGITATION :-
- Regurgitation means backward flow of
blood from aorta into left ventricle during diastole due to damage to the aortic valve.
⭐⭐⭐⭐⭐⭐
3) ETIOLOGY OF AORTIC REGURGITATION:-
(a) Acute causes :-
(I) Rheumatic fever :-
- Rheumatic fever is an autoimmune inflammatory disease which affects many connective tissues including heart.
- It causes inflammation and
damage to aortic valve.
(II) Infective endocarditis :-
- It is the infection of heart valves
and endocardium caused by
bacteria, fungi or rickettsia.
- Organisms can infect already
damaged heart valves (less
virulent organisms) or normal
heart valves ( more virulent
organisms)
(III) Trauma to the aortic valve
(IV) Dissecting aneurysm of aorta -
- There is tear in the inner layer of
aorta due to causes like high BP,
atherosclerosis ,etc.
- Blood enters the tear and causes
seperation of inner and middle
layers of aorta .Blood starts
accumulating between these two
layers.
- The unsupported intimal flap which
is formed due to accumulation of
blood prolapses sags and crosses the aortic valve.
- The swinging motion of the
unsupported intimal flap through
the aortic valve causes regurgitation
(b) Chronic causes :-
(I) Common causes:-
# Rheumatic fever - It can be acute
as well as chronic cause.
# Atherosclerotic aortic valve :- there
is chronic inflammation, lipid
deposition, thickening of fibrosa
layer and hence damage to valve.
# Syphilis - There is dilatation of
aortic ring with incompetence of
the valve due to inflammation.
# Bicuspid aortic valve - Normally,
aortic valve has 3 cusps. But in
case of Bicuspid valve, there are
only 2 cusps. Third leaflet doesn't
develop properly. This abnormal
valve causes regurgitation as it
doesn't close properly.
(II) Uncommon causes :-
# Infective endocarditis - can be
acute as well as chronic cause.
# SLE ( systemic Lupus
erythematous) - It is Autoimmune
disease. It can cause inflammation
in the heart valve and can damage
it.
# Ankylosing spondylitis :- It is
autoimmune and chronic
Inflammatory disease which affects
joints. It can also affect heart .
# Reiter syndrome :- It is an
autoimmune response to Infections
like gastrointestinal infection. The
inflammation can spread to heart.
# Takayasu syndrome - It is a rare
autoimmune disease which causes
inflammation of large arteries.
# Ehler Danos syndrome :- It is an
inherited disorder which mostly
affects connective tissue of skin,
joints, blood vessels, heart valves,
etc. There is problem in formation of
collagen, thus connective tissue
formation is affected.
# Marfan syndrome :- It is autosomal
dominant disease with mutation in
FBN1 gene. It causes dilatation of
the aortic root. This dilatation leads
to stretching of the aortic valve
cusps and hence the valve fails to
close.
# Hypertension :- the pressure causes
direct damage to the valve leading to
fibrosis and stiffening of valve.
# Rheumatoid arthritis - It is an
autoimmune and inflammatory
disease . It can cause inflammation
and damage to the arteries and
heart valves.
# Aortic aneurysm :- weak spot in
the aortic wall begins to bulge. This
leads to increased pressure of blood
over the aortic valve and causes
damage to the valve. There is also
risk of aortic dissection.
# Ventricular septal defect (VSD) :-
Note - Venturi effect states that
velocity of a fluid passing through
constricted area will increase and
it's static pressure will decrease.
Similarly , blood flowing through
VSD from left ventricle to right
ventricle flows with increased speed
and decreased pressure.
This decreased pressure causes
prolapse of the aortic valve and
it's inability to close thus causing
regurgitation.
⭐⭐⭐⭐⭐⭐
4) PATHOPHYSIOLOGY OF AORTIC REGURGITATION :-
(I) Due to regurgitation, some amount
of blood enters the left ventricle from the aorta during the diastole. Thus, end diastolic volume of left ventricle increases. This causes dilatation of left ventricle. As a result, the stroke volume increases. (Frank Starling's law states that the stroke volume of the left ventricle will increase as the left ventricular volume increases due to the muscle stretch causing a more forceful systolic contraction)
However, efficiency of left ventricle decreases gradually & stroke volume decreases.This results in further dilatation & finally Left Ventricular Failure.
(II) Due to left ventricular failure , there is backpressure into the left atrium leading to rise in left atrial pressure, then pulmonary venous pressure, the pulmonary artery pressure and lastly pressure in the right heart increases.
5) SYMPTOMS OF AORTIC REGURGITATION :-
(I) Initially asymptomatic.
(II) Palpitations, Pulsations in neck -
due to increased stroke volume because
of increased force of pumping. (Frank
Starling law)
(III) Angina -
As efficiency of left ventricle
decreases, cardiac output decreases which decreases the blood flow to the coronary artery leading to Angina.
(IV) Syncope - Decreased efficiency of left ventricle leads to decreased cardiac output and hypotension which leads to
loss of consciousness. It is seen
afterwards.
(V) Dyspnea (exertional) - As the LV end-
diastolic pressure increases rapidly, there is increase in pulmonary venous pressure . As pressure increases throughout the pulmonary circuit, the patient develops dyspnea. Also, decreased pumping efficiency causes
decreased oxygen supply to tissues
(VI) Orthopnea - it occurs due to pulmonary congestion in supine position. It occurs because in supine position there is redistribution of blood volume from the lower extremities and
splanchnic vessels to the lungs. In case of AR, this redistribution of blood worsens the already present pulmonary congestion.
(VII) Signs of Right ventricular failure -
Seen late - see pathophysiology.
⭐⭐⭐⭐⭐⭐⭐
6) SIGNS OF AORTIC REGURGITATION:-
(I) Rosenbach sign - Increased liver
pulsations during systole. It is caused
due to increased stroke volume.
(II) Gerhardt sign - Increased spleen
pulsations due to increased stroke
volume.
(III) Muller sign - Increased uvula
pulsations due to increased stroke
volume.
(IV) Becker sign - Increased retinal
artery pulsations.
(V) Landolfi sign - Alternate
constriction & dilatation of pupil with
cardiac cycle.
During systole the stroke volume
increases which leads to increase in
systolic B.P. Thus, parasympathetic
response gets activated to decrease the
B.P. It also leads to constriction of
pupil.
During diastole, stroke volume
decreases which leads to decrease in
BP. Thus, sympathetic response is
activated to increase the BP It also
leads to dilatation of pupil.
(VI) Quinke's sign - When nail bed is
pressed slightly, there is alternate
flushing & paleness of nailbed with
cardiac cycle , i.e. flushing during
systole (increased stroke volume) &
paleness during diastole.
(VII) Pistol Shot femoral sign - Boom
like systolic pulsations in femoral
artery.
(VIII) Wide pulse pressure -
Pulse pressure = Systolic BP - diastolic
BP.
It is increased in aortic regurgitation
because
- the systolic pressure is increased
due to increased stroke volume.
- diastolic pressure is decreased
because some blood regurgitates
back into the left ventricle thus
decreasing diastolic blood volume
in the systemic circulation.
(IX) Hills sign - The systolic BP at the
popliteal artery is more than the
brachial artery.
Reason - The lower limb vessels are
a direct continuation of aorta unlike
upper limb vessels.
(X) Waterhammer pulse - Collapsing
Pulse.
- Arm is elevated & pulse is felt in the
radial artery. There is high upstroke
& high downstroke.
- It is bounding, forceful pulse with a rapid upstroke and descent.
- Eg. There is a tube filled with some
water. There is vaccum inside the
tube. When it is inverted, the water
hits the bottom of the tube with
force - Water hammer hitting like
sound.
- In aortic regurgitation, increased
stroke volume causes rapid
upstroke.
- In similar way, the diastolic pressure
in the arm is decreased because some blood regurgitates
back into the left ventricle thus
decreasing diastolic blood volume
in the systemic circulation. This leads
to rapid emptying of arterial system
& thus rapid downstroke.
(XI) Corrigan sign - Similar to
Waterhammer, but felt in carotid
artery.
(XII) De Musset sign - Anteroposterior
movement of head as per cardiac
cycle.
⭐⭐⭐⭐⭐⭐
7) INSPECTION & PALPATION :-
(I) Hyperdynamic precordium & apex - precordium moves too much ( due to increased forceful pumping and increased stroke volume )
(II) Pulsations in neck, carotid thrill,
pulsation in suprasternal area.( due to increased forceful pumping and increased stroke volume )
⭐⭐⭐⭐⭐⭐
8) AUSCULTATION :-
These diagrams will be helpful for understanding if information given below is difficult to understand.
(I) S1 -
Normally, it occurs due to closure of bicuspid, tricuspid valves at the beginning of systole to prevent the entry of blood from ventricles back into the atria.
S1 is normally a single sound because mitral and tricuspid valve closure occurs almost simultaneously.
# In aortic regurgitation, S1 may be soft because as the left ventricular end diastolic volume goes on increasing due to regurgitant blood, left ventricular pressure rises earlier than the normal time required. This elevated pressure in the left ventricle causes premature closure of mitral valve during diastole only (still systolic phase is yet to come) whereas normal closure of mitral valve occurs at the beginning of systole. Hence Sound may be soft .
(II) S2 -
Normally, it occurs due to closure of semilunar valves i.e aortic and pulmonary valves at the end of ventricular systole and beginning of diastole to prevent the entry of blood from aorta and pulmonary artery back into the ventricles.
S2 is normally split because the aortic valve (A2) closes before the pulmonary valve (P2) because the closing pressure i.e diastolic arterial pressure is aorta than the pulmonary artery .In addition, the more muscular and stiff and less compliant left ventricle (LV) empties earlier than the right ventricle.
In the normal heart:
During expiration:
The second sound (S2) appears usually single because the split is very narrow.
During inspiration:
The second sound (S2) appears to be made of two component sounds:
Aortic valve closure (A2) which happens first.
Pulmonic valve closure (P2) which happens second.
Explaination is as follows:-
The venous return to the right ventricle (RV) increases during inspiration due to negative intrathoracic pressure. Hence, volume of blood in right ventricle increases and more time is required to empty the right ventricle.Therefore, P2 is even more delayed. So the split of the second heart sound widens during inspiration and narrows during expiration.
#In Aortic regurgitation,
- S2 may be single or narrow splitting or paradoxical splitting may be present.
- Single S2 indicates that there is absence of A2 i.e failure of aortic valve to close due to damage to the valve.
- Narrow splitting indicates that there may be delayed closure of aortic valve as in case of aortic regurgitation due to damaged valve.
- Paradoxical splitting of S2 (P2 is heard before A2)
Aortic valve (A2) closes after the pulmonary valve (P2).A paradoxical split S2 occurs in cases where there is delay in the closure of aortic valve as in case of aortic regurgitation.
Since the respiration only affects P2 (i.e negative intrathoracic pressure during inspiration increases the venous return in right ventricle and thus delays P2) its effect in paradoxical splitting is the opposite of normal, i.e. inspiration causes narrow splitting while expiration causes wide splitting of S2
- paradoxical split S2 heart sound occurs when the splitting is heard during expiration and disappears during inspiration — opposite of the physiologic split S2.
- In Rheumatic heart disease , there is soft A2 and in syphilis,there is loud A2.
(III) S3 - (The third heart sound (S3), also known as the “ventricular gallop,” occurs just after S2 . It occurs due to opening of the mitral valve which allows passive filling of the left ventricle during start of diastole. The S3 sound is produced by the large amount of blood striking a very compliant left ventricle. Compliance means how easily the ventricle expands.)
# In aortic regurgitation, S3 is present in patients with left ventricular failure because in case of ventricular failure, the ventricle becomes dilated and overly compliant.
(IV) S4 -( S4 sound occurs due to atrial contraction in the late diastolic phase .It occurs due to vibration of the ventricular wall during atrial contraction. The sound is associated with a stiffened ventricle due to low ventricular compliance.Therefore it is seen in case of ventricular hypertrophy.)
# In aortic regurgitation, S4 is seen in patients with left ventricular
hypertrophy.
(V) Early diastolic regurgitant murmur -
(Due to backflow from aorta into left
ventricle during start of diastole)
Heard good when patient sits, leans
forward, breath held at deep expiration
& hands clenched. It is heard best at the left third intercostal space called erb's point. Soft type in rheumatic
disease & 'seagull' type in syphilis.
(VI) Mid diastolic murmur - severe
cases of regurgitation. It indicates that regurgitation which had started in the beginning of diastole is still present during mid diastole also because of more severe damage to aortic valve.
(VII) Ejection systolic murmur -
In case of AR, there is increased stroke volume due to increase in end diastolic volume in left ventricle. This increased stroke volume causes ejection systolic murmur.
⭐INVESTIGATIONS AND TREATMENT ARE WRITTEN IN COMMENT SECTION.⭐
⭐⭐⭐⭐⭐⭐⭐
9) INVESTIGATIONS OF AORTIC
REGURGITATION :-
(I) Echocardiography.
(II) Doppler Echocardiography.
(III) Cardiac catheterization.
(IV) Coronary Angiography.
(V) VDRL - for Syphilis.
(VI) RA factor, ANA, CRP - for
connective tissue disorder.
(VII) ECG.
(VIII) Chest X-ray - Pulmonary edema,
Cardiomegaly (Left Ventricle)
⭐⭐⭐⭐⭐⭐⭐
10)TREATMENT OF AORTIC REGURGITATION :-
(I) Treat the cause.
(II) Prophylaxis of Rheumatic fever.
(III) Treatment of Heart failure -
# Digoxin - It strengthens the force of the heart muscle's contractions, helps restore a normal, steady heart rhythm
# Diuretics - Diuretics help the kidneys get rid of unneeded water and salt. This makes it easier for your heart to pump
# Salt & Fluid Restriction - to prevent
overload on heart.
(IV) Reduction of After load -
# Isosorbide Dinitrate - it causes
arterial relaxation & dilatation.
# Hydralazine -Causes Vasodilation.
# Captopril - Causes Vasodilation.
(V) If asymptomatic & normal LV
function -
# No surgery required.
# Only monitoring is done.
(VI) If systolic LV ejection fraction <50%
& end diastolic LV diameter >55 mm.
# AORTIC VALVE REPLACEMENT
surgery is done.
⭐⭐⭐⭐⭐⭐












Very nicely and detailed explanation
ReplyDeleteVery nice & informative article. 🙂👍👍👍👌👌👌 Keep it up Dr.Nikita
ReplyDeleteThank you so much 😊😊
DeleteExplanation level 100!
ReplyDeleteDifficult topic explained in very easy language 👌👌 Well done Dr. Nikita
Thank you so much 😊😊
DeleteGood work👌
ReplyDeleteThank you so much 😊😊
Delete
ReplyDelete9) INVESTIGATIONS OF AORTIC
REGURGITATION :-
(I) Echocardiography.
(II) Doppler Echocardiography.
(III) Cardiac catheterization.
(IV) Coronary Angiography.
(V) VDRL - for Syphilis.
(VI) RA factor, ANA, CRP - for
connective tissue disorder.
(VII) ECG.
(VIII) Chest X-ray - Pulmonary edema,
Cardiomegaly (Left Ventricle)
⭐⭐⭐⭐⭐⭐⭐
10)TREATMENT OF AORTIC REGURGITATION :-
(I) Treat the cause.
(II) Prophylaxis of Rheumatic fever.
(III) Treatment of Heart failure -
# Digoxin - It strengthens the force of the heart muscle's contractions, helps restore a normal, steady heart rhythm
# Diuretics - Diuretics help the kidneys get rid of unneeded water and salt. This makes it easier for your heart to pump
# Salt & Fluid Restriction - to prevent
overload on heart.
(IV) Reduction of After load -
# Isosorbide Dinitrate - it causes
arterial relaxation & dilatation.
# Hydralazine -Causes Vasodilation.
# Captopril - Causes Vasodilation.
(V) If asymptomatic & normal LV
function -
# No surgery required.
# Only monitoring is done.
(VI) If systolic LV ejection fraction <50%
& end diastolic LV diameter >55 mm.
# AORTIC VALVE REPLACEMENT
surgery is done.
⭐⭐⭐⭐⭐⭐
Very nice👌
ReplyDeleteBahot acche betaji
ReplyDeleteThank you so much 😊😊
Deleteলেখার দক্ষতা খুব সুন্দর
ReplyDeleteThank you so much 😊😊
DeleteArticle is very nice 👍👍
ReplyDeleteThank you so much 😊😊
DeleteVery much impressed!
ReplyDeleteThank you so much 😊😊
Deleteखास👌
ReplyDeleteThank you so much 😊😊
Deleteखुप छान बेटा👌 अवघड विषय असून
ReplyDeleteअप्रतिम लिखाण व प्रस्तुति
Thank you so much 😊😊
Deleteكنت أبحث عن هذا الموضوع منذ وقت طويل. هذا هو أفضل مقال. شكرا سيدتي.
ReplyDeleteبارك الله فيكم وعلى والديك ، ووفقكم الله خيرًا. أحبك الهند.
د.محمد صلاح
Thank you so much for your appreciation 😊😊
DeleteIt means a lot on occasion of independence day of India ☺️☺️
DeleteImpressive!
ReplyDeleteThank you so much 😊😊
Deleteعيد استقلال سعيد يا دكتور نيكيتا
ReplyDeleteThank you so much 😊😊
Delete👌👌
ReplyDeleteThank you so much 😊😊
DeleteVery very good. I m so impressed!
ReplyDeleteThank you so much 😊😊
DeleteGreat
ReplyDeleteThank you so much 😊😊
DeleteWow👌👌
ReplyDeleteThank you so much 😊😊
Deleteअप्रतिम👍
ReplyDeleteBadhiya
ReplyDeleteThank you so much 😊😊
DeleteClassic. Loved very much
ReplyDeleteThank you so much 😊😊
DeleteBeautifully written!
ReplyDeleteThank you so much 😊😊
DeleteLoved it very much, especially the auscultation part. Thank u dr madam
ReplyDeleteThank u so much 😇
DeleteWriting best
ReplyDeleteThank you so much 😊😊
Deletehow can someone make things so simple! amazed! esp. S1 S2 part👌
ReplyDeletedr.Nikata Vineyak , hatts off.
Josh Cumberbatch (GradeV Brighton & Sussex Medical School, UK)
Thank you so much 😊😊
DeleteGood
ReplyDeletePerfect Presentation
ReplyDeleteThank you so much 😊😊
DeleteVery well done
ReplyDeleteThank you so much 😊😊
DeleteVeey good
ReplyDeleteThank you so much 😊😊
DeleteWell done niketa
ReplyDeleteThank you so much 😊😊
DeleteI not understand AR in my medical school when my professor teach.But Prof. Dr. Nikita Vinayak medam explained in magical way. So easy. I m your fan medam. I love India for Shehrukh Khan & Hydirabadi Biryeni, now you too are my favorites in India medam. I m amazed how intelligent Indians are! ❤️
ReplyDeleteFatima Ramshad Albdulwahid, West Jakarta.
Thank you so much 😊😊 but I am not a professor .I am doing internship after MBBS.
DeleteThank you very much for your appreciation and support 😊😊
DeleteThank you so much 😊😊
ReplyDelete👍
ReplyDeleteThank you so much 😊😊
DeleteBahot accha likhti ho aap👌
ReplyDeleteThank u so much 😇
DeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteNice
ReplyDeleteThank you so much 😊😊
Deleteबेटा, नेहमीप्रमाणे अप्रतिम लिहलस👌👌
ReplyDeleteतू कुठली आहेस?
Thank you so much 😊😊 I am from sangli
DeleteThank you so much 😊😊
ReplyDeleteमी वाशिम ची आहे बेटा.
ReplyDeleteHo mahit ahe madam😊
Deleteकाफी पसन्द आया
ReplyDeleteThank you so much 😇
DeleteI have read most of your blogs. I am very impressed by the way you present it & explain it.
ReplyDeleteYour pointwise explanation & ease of language has left me speechless.
You are really a dedicated person who enlighten us by your knowledge. I have been a Dr. all my life & know very well that the job is not very easy. Despite this, your dedication has amazed me.You do your work as well as share this valuable knowledge with us regularly.You remind me of my grand daughter who used to write medical blogs but met with an accident last christmas & passed. I wish I should have appreciated her when she was with me.
I know appreciation acts as an Adrenaline shot to a budding writer which is as rare as a gem nowadays.
I rarely comment on articles but I am forced to tell you this because I have seen the unique writing skill in you.
Please keep on going. Never fall down whatever people say.
You are doing very good work my child.
See you soon.
Your grandpa from Berlin
Dr. William Orton.
I am very much happy for this valuable appreciation sir.
DeleteYour words meant a lot for me. I really felt inspired by your words. Keep blessing and supporting your granddaughter from India ☺️☺️ Thank you
Thank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteThis comment has been removed by the author.
ReplyDeleteRead all pots
ReplyDeleteThank you so much 😊😊
DeletePosts
ReplyDeleteThank you so much 😊😊
DeleteCommented on all posts
ReplyDeleteThis comment has been removed by the author.
DeleteThank you so much for reading and appreciation 😊😊
DeleteVery nice writing
ReplyDeleteThank you so much 😊😊
DeleteKeeep it up
ReplyDeleteThank you so much 😊😊
DeleteDr.Nikipatil is the best
ReplyDeleteThank you so much for much needed support and appreciation 😊😊
DeleteCardio was awesome as others
ReplyDeleteThank you so much 😊😊
Delete