⭐NEPHROTIC SYNDROME ⭐
⭐NEPHROTIC SYNDROME ⭐


A disorder of kidney which is characterized by Proteinuria, Oedema, Hypoalbuminemia ,Hyperlipidemia and sometimes Hypertension.
( #Proteinuria - presence of abnormal quantities of protein in urine.
# Hypoalbuminemia - decreased levels of
albumin in blood.
# Oedema - swelling caused by build up
of fluid.
# Hyperlipidemia - Increased levels of
lipids in blood.
# Hypertension - high blood pressure.)
⭐⭐⭐⭐⭐
1) PATHOPHYSIOLOGY of nephrotic syndrome:-
(A) In nephrotic syndrome, there is
increase in permeability of
glomerular capillaries which leads to
proteinuria.
This increase in permeability may be
due to :-
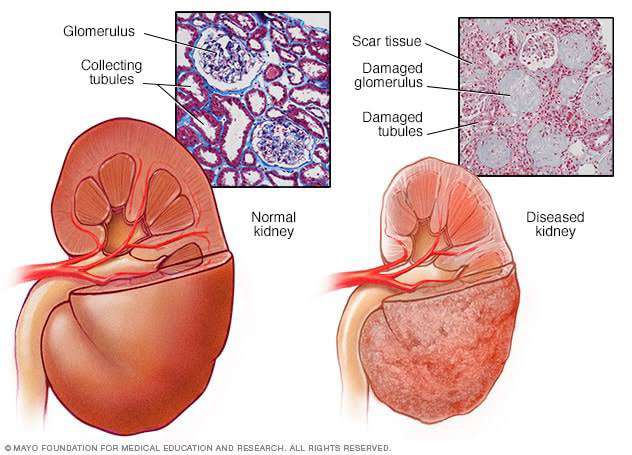
(I) Glomerular inflammation - there is
damage to glomeruli due to
cytokines and permeability factors
released during inflammation.
(II) Change in charge of GBM i.e
glomerular basement membrane.
- Normally it has net negative
charge and hence repels
negatively charged albumin.
- change in charge can lead to
decreased repulsion and hence
can cause proteinuria.
(III) # Change in size of filtration slits
in Bowman's capsule -
( Podocytes are specialized cells
lining visceral layer of Bowman's
capsule. Foot processes of
podocytes wrap themselves
around capillaries of glomerulus
to form filtration slits through
which ultrafiltration of blood
occurs.)
# Increase in the size of filtration
slits leads to filtration of proteins
like albumin.
# This increase in size occurs due
to deformation of podocyte foot
processes which may occur due
to mutation of podocyte proteins.
(B) # Proteinuria - Occurs due to
increased glomerular permeability.
# Hypoalbuminemia - due to loss of
albumin through urine.
# Oedema - Due to decreased level
of albumin in blood, plasma oncotic
pressure decreases and fluid goes
from intravascular compartment to
extravascular compartment leading
to oedema.
# Hyperlipidemia - Due to
(I) Hypoalbuminemia causes
upregulation of HMG CoA
reductase enzyme which is involved
in cholesterol synthesis and it also
causes downregulation of enzyme
lipoprotein lipase which degrades
lipoprotein. Thus, lipids increase
leading to Hyperlipidemia.
(II) Kidneys are major site of
metabolism of mevalonate ,a
precursor in cholesterol synthesis.
This metabolism and excretion of
mevalonate is impaired in
nephrotic syndrome due to
damage to kidney. Hence,
increased mevalonate causes
increased cholesterol synthesis in
liver leading to Hyperlipidemia.
# Hypertension - It may occur sometimes due to RAAS activation as intravascular volume decreases due to shift of fluid into extravascular compartment.
⭐⭐⭐⭐⭐⭐
2) EFFECTS OF LOSS OF PROTEINS in
Nephrotic syndrome :-
(A) Due to loss of thyroxine binding
protein - thyroid problems may occur.
(B) Loss of calciferol binding protein-
Vit D deficiency may occur.
(C) Loss of metal binding protein -
metal deficiency.
(D) Loss of transferrin - anemia
( Transferrin helps in iron transport)
(E) Loss of drug binding protein-
defective pharmacokinetics of drugs
(F) Loss of albumin - leads to edema,
ascites, pleural effusion, subungual
edema ( beneath nail beds)
(G) Loss of Globulin- decreased formation of IgG leading to bacterial
peritonitis.
(H) Loss of antithrombin- Hypercoagulable state, renal vein thrombosis.
(Other causes of hypercoagulable state= Altered levels of protein C & S), increased hepatic production of fibrinogen.)
Renal vein thrombosis can cause flank
pain, hematuria, MI, stroke, pulmonary embolism
⭐⭐⭐⭐⭐
3) CAUSE Of Nephrotic syndrome:-
(A) Primary Glomerular Disease (Idiopathic)=
i) Minimal Change Disease: Most common cause of nephrotic syndrome in children which is caused due to effacement (erased or blotting out )of podocyte process.
(Foot processes of podocytes spread & form mesh like network. Pores in between them form filtration slits. In minimal
change disease, there is altered T cell mediated immunological response leading to abnormal secretion of lymphokines by T cells causing effcaement of foot processes. Hence, steroids are given to suppress this immune response.)
ii) Focal & Segmental Glomerulosclerosis.
iii) Membranous GN.
iv) Mesangial Proliferative Glomerulonephritis.
B) Secondary Causes=
i) Infections:
(Can cause kidney injury by direct invasion or by cytokine based & immune based mechanism leading to increased glomerular permeability).
HIV, syphilis, Hep B, Malaria, Leprosy, infective endocarditis.
ii) Tumors: Hodgkin's Lymphoma, Carcinoma, Leukemia.
(Due to infiltration of tumor cells in kidney, inflammation & increased permeability may occur. Also tumor antigen deposition may occur.)
iii) Metabolic:
#Diabetes (Increased blood glucose leads to increased blood flow to the kidney for increased excretion of glucose leading to strain & damage to glomeruli.)
#Amyloidosis.
iv) Connective tissue disorders:
SLE, Rheumatoid Arthritis.
(Autoantibodies affect kidney leading to inflammation.)
v) Drugs & toxins:
(cause inflammation to kidney)
Heroin, Mercury, Gold, Penicillamine, Captopril.
⭐⭐⭐⭐
4) INVESTIGATIONS of nephrotic syndrome:-
A) 24 hr urinary protein measurements=
(detects proteinuria).
B) Serum Albumin=
(Detects hypoalbuminemia).
C)Serum Cholesterol=
(Detects hyperlipidemia).
D) Sometimes Red cell casts may be present in urine microscopy.
E) Renal biopsy.
F) Appropriate investigations for secondary causes.
. ⭐⭐⭐⭐
5) TREATMENT of nephrotic syndrome:-
A) t/t for proteinuria=
i)ACE inhibitors :
(MOA= Normally, Angiotensin II causes efferent arteriolar vasoconstriction which causes increased glomerular hydrostatic pressure leading to proteinuria. ACE inhibitors prevents this by causing afferent & efferent vasodilation).
ii)NSAIDS:
(MOA= Prostaglandins cause afferent arteriolar vasodilation causing increased amount of blood reaching glomeruli and thus increasing glomerular blood pressure. NSAIDS prevent PG production and hence cause afferent arteriolar vasoconstriction thus decreasing glomerular blood flow. However risks of vasoconstriction are ARF, hyperkalemia, salt retention).
B) t/t for preventing complications=
i)Vit. D = treats deficiency .
ii) Anticoagulants = for thrombosis.
iii) Cholesterol lowering drugs = for hyperlipidemia.
iv) Dietary protein = 0.8 to 1 g/kg, not more to prevent renal failure.
v) Salt restriction & diuretics = treats edema.
vi) Sometimes i.v. Albumin is given.
C) t/t of Cause=
i)Minimal Change Disease:
In patients, Corticosteroids like Prednisolone in a dose of 60 mg/m2 daily for 4 weeks & 35 mg/m2 on alternate day for next 4 weeks.
a)Children who respond: Steroid Responders.
b)Children who show relapse on withdrawal of drug: Steroid dependent syndrome. They are given drugs as initial regimen & there by tapering regimen very slowly.
c)Other drugs: Cyclosporine, Tacrolimus, Cyclophosphamide.
ii) Membranous GN: Steroids in combination with cyclophosphamide & cyclosporine.
⭐⭐⭐⭐⭐⭐⭐⭐

Difficult topic made easy 👌👌
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeletePathogenesis & Treatment very well explained!!👌👌Keep it up dear.
ReplyDeleteThank you so much 😊😊
Deleteलिखाणाची शैली खूपच सुंदर 👌
ReplyDeleteखूप खूप आशीर्वाद बेटा😊
Thank you so much 😊😊
DeleteMy son who's a medical student at Tver State Medical University had difficulty in understanding Nephrotic syndrome. This article is the easiest & best compilation amongst what we searched. Thanks Doc.❤️
ReplyDeleteBahot khub madamji👌👌
ReplyDeleteLove from Bihar❤️
Thank you so much 😊😊
DeleteWell done👌
ReplyDeleteThank you so much 😊😊
DeleteEtiopathogenesis mind blowing explanation 👌
ReplyDeleteVery nice👌
ReplyDeleteThank you so much😊😊
DeleteGood to see a budding writer with marvellous writing skills!
ReplyDeleteJacob K. ,MD. (Southampton)
Thank you so much sir for reading 😊😊
DeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDeleteThank you so much 😊😊
ReplyDelete👌👌
ReplyDeleteThank you so much 😊😊
DeleteLoved it
ReplyDeleteThank you so much 😊😊
DeleteBlog is such a beauty 👌
ReplyDeleteArticles are to the point
ReplyDelete❤️ from Istanbul dr
Thank you so much for reading 😊😊
DeleteGreat
ReplyDeleteWell done dr nikata❤️
ReplyDelete👌👌👌👌बेस्ट
ReplyDeleteThank you so much 😊😊
DeleteGood to see an independent woman writing👌
ReplyDeleteThank you so much 😊😊
Delete👍
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeleteWelll done
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDeleteGoooooood
ReplyDeleteThank you so much 😊😊
DeleteBest
ReplyDeleteThank you so much 😊😊
DeleteThank you so much 😊😊
ReplyDelete👌
ReplyDeleteThank you so much 😊😊
ReplyDeleteमस्त
ReplyDeleteThank you so much 😊😊
Delete